

My daughter had her first cavity at age four. I was mortified. We brushed her teeth every night or at least I thought we did a decent job. Her pediatric dentist sat me down and said, very gently, “Have you been using fluoride toothpaste? And are the amounts right for her age?”
I had no idea there was a “right amount.” I’d been using a pea-sized glob since she was one year old, which turns out is way too much for a toddler. And before that? Just water on the brush, because I’d read somewhere online that fluoride might be dangerous for babies.
That appointment changed how I thought about fluoride entirely. And since then, I’ve talked to enough parents in waiting rooms and online communities to know I wasn’t alone in my confusion.
So let’s break this all down to what fluoride actually does, how it’s used in pediatric dentistry, how much is right for each age, and what mistakes most parents (including me) make without even realizing it.
What Fluoride Actually Does in a Child’s Mouth
Here’s the thing most people get backwards: fluoride doesn’t just “strengthen teeth.” It’s more active than that.
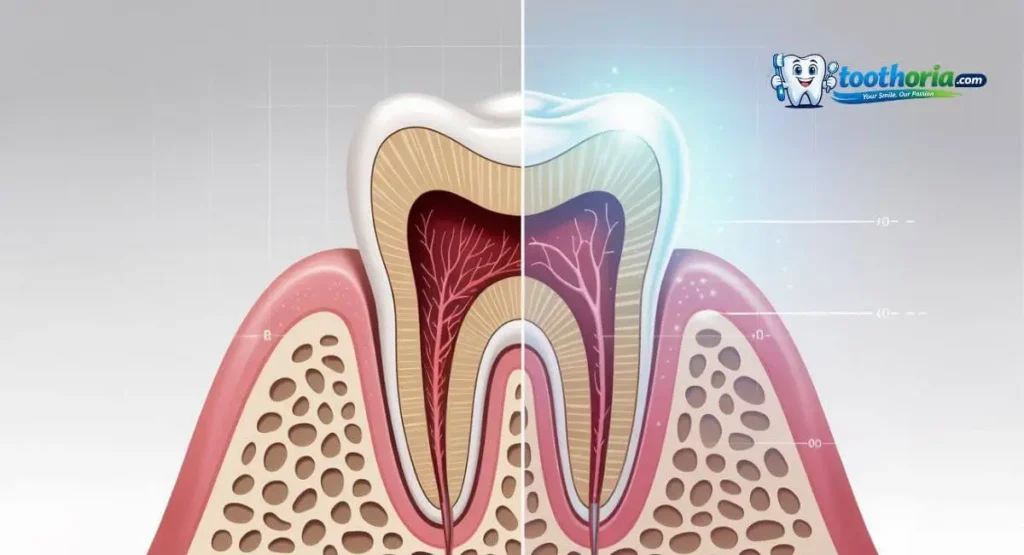
Every single day, the bacteria in your child’s mouth eat the sugars they consume and produce acid as a byproduct. That acid eats away at tooth enamel in a process called demineralization. Fluoride intervenes in two important ways:
- It speeds up remineralization; it helps pull calcium and phosphate back into the enamel, literally repairing early damage before a cavity forms.
- It makes enamel more acid-resistant when fluoride becomes part of the tooth’s crystal structure (forming fluorapatite), it’s harder for acid to break down.
For kids, this is especially significant because their enamel is less mature and more porous than adult enamel. They’re eating constantly, snacking between meals, often not rinsing well, and going hours without saliva production when they sleep. Their teeth are in a near-constant state of acid attack.
Fluoride is the single most evidence-backed intervention in pediatric dental care. The American Academy of Pediatric Dentistry (AAPD) has supported its use for decades, and the science keeps affirming it.
When Does Fluoride Use Start? (By Age, With Real Guidance)
This is where most parents get confused, because the recommendations changed significantly in 2014 and a lot of older parenting blogs still have the old info floating around.
Infants (Birth to 12 Months)
Your infant doesn’t need fluoride toothpaste yet they don’t have teeth. But here’s something worth knowing: if your home uses well water, your baby may not be getting any fluoride from drinking water, which matters more as teeth start coming in.
Use a soft, wet cloth to clean their gums after feeding. No toothpaste at this stage.
Toddlers (12 Months to 36 Months)
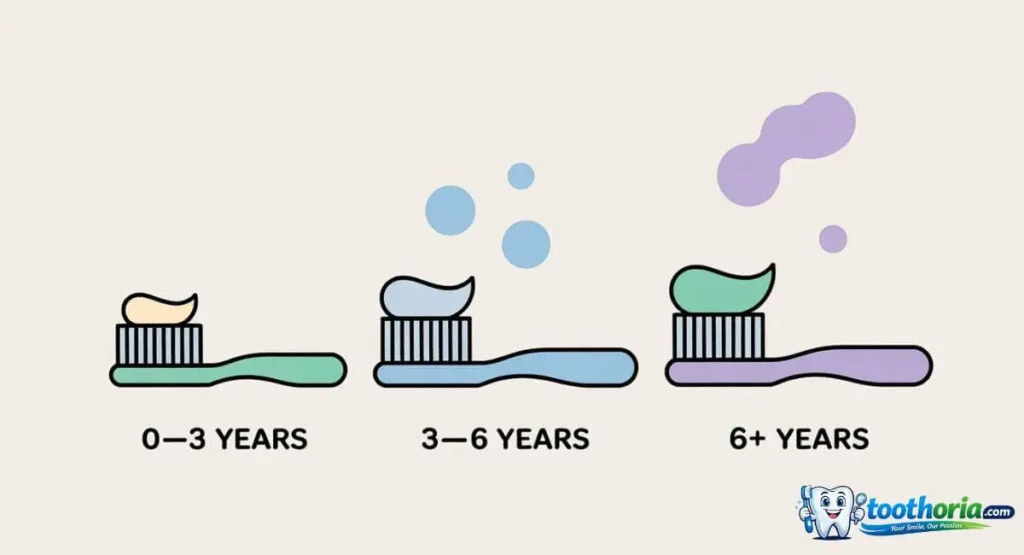
This is where the updated guidance changed things. The AAPD now recommends that as soon as the first tooth appears, you start brushing with a smear of fluoride toothpaste the size of a grain of rice. Not a pea. A grain of rice.
The reason for the tiny amount isn’t because fluoride is dangerous in small doses it’s because toddlers swallow almost everything, and excessive ingestion over time can affect developing teeth (a condition called dental fluorosis, which I’ll cover below).
A rice-grain smear twice a day at this age is both safe and effective.
Preschoolers (3 to 6 Years)
Once a child can reliably spit (usually around age 3), you move up to a pea-sized amount of fluoride toothpaste. This is the amount most adults are familiar with, and yes, it’s appropriate even for a four-year-old as long as they’re spitting afterward, not swallowing.
I made the mistake of using a pea-sized amount before my daughter could spit. Nobody told me. Don’t make the same mistake.
School-Age Children (6 and Up)
By six or seven, most kids have the motor skills and the sense to spit properly. You continue with a pea-sized amount of fluoride toothpaste. This is also the age when dentists may start recommending fluoride rinses for kids at higher cavity risk.
Fluoride Treatments at the Dentist’s Office

Beyond what you do at home, pediatric dentists have several professional fluoride options that are significantly stronger than anything available over the counter.
Fluoride Varnish
This is the most common in-office treatment for young children, and if you’ve ever taken your kid to the dentist and seen them paint something on their teeth at the end of the visit, this is what that was.
Fluoride varnish is a sticky, concentrated fluoride that gets painted directly onto the teeth with a small brush. It sets on contact with saliva and continues releasing fluoride for several hours afterward. The taste is usually mild, it’s not uncomfortable, and kids tolerate it well.
The AAPD recommends fluoride varnish every 3 to 6 months for children at moderate to high cavity risk. Even the American Academy of Pediatrics now recommends that primary care pediatricians apply fluoride varnish at well-child visits starting at the first tooth not just dentists.
My daughter gets varnish at every six-month checkup. It takes about two minutes. I notice a visible difference in how her teeth look after slightly glossier for a day or two.
Fluoride Gel and Foam
For older children (usually 6 and up who can hold a tray in their mouth without swallowing), dentists use fluoride gel or foam applied in a mouth tray for about four minutes. These are higher concentration treatments than varnish and work well for kids who’ve had multiple cavities or who are in orthodontic treatment with brackets and wires that trap plaque.
Silver Diamine Fluoride (SDF)
This one deserves its own section because it’s genuinely changed pediatric dentistry in the last decade, and most parents have never heard of it.
Silver diamine fluoride is a liquid that combines silver (antimicrobial) and fluoride (remineralizing) in one solution. Applied directly to a cavity, it can actually arrest the decay meaning it stops the cavity from growing without any drilling.
The main downside: it permanently stains the treated decay black. The silver oxidizes and turns dark. That’s not harmful, and it’s not visible on back teeth, but it’s cosmetically noticeable on front teeth, which makes SDF a conversation parents need to have with their dentist before deciding.
For kids who are too young or too anxious for conventional fillings, or for families navigating cost issues, SDF can be an incredible option. If your child’s dentist has never mentioned it, it’s worth asking about especially for cavities in baby teeth that are going to fall out anyway.
Fluoridated Water: The Invisible Benefit
Before in-office treatments and toothpaste, there’s fluoridated municipal water and it still does meaningful work.
Community water fluoridation has been ongoing in the US since 1945 and is considered one of the ten greatest public health achievements of the 20th century by the CDC. The current recommended level is 0.7 milligrams per liter.
When kids drink fluoridated water, they get continuous low-level fluoride exposure throughout the day. Saliva naturally distributes it across tooth surfaces. It’s passive, easy, and clinically effective at reducing cavities.
If you use well water or a private water source, your dentist may recommend fluoride supplements prescription drops or tablets to compensate. These are not OTC products; your child’s pediatrician or dentist will assess the fluoride level in your local water before prescribing.
If you use a reverse osmosis filter at home, know that it removes fluoride. Some parents prefer this for other health reasons, which is a personal choice but it’s worth discussing with your dentist so they can adjust their recommendations accordingly.
Dental Fluorosis: The Risk Parents Worry About

Let’s address the concern that drives most of the anti-fluoride parenting content online.
Dental fluorosis is a cosmetic condition that can occur when a child ingests too much fluoride during the years when their permanent teeth are forming (roughly birth to age 8). The effects range from barely visible white spots on the enamel to, in severe cases, pitting and brown staining.
Here’s the important context: the vast majority of fluorosis cases in the US are mild white spots that are cosmetically subtle and don’t affect the function or health of teeth at all. Severe fluorosis is rare and is associated with very high fluoride ingestion, usually from fluoride supplements combined with heavily fluoridated water, not from toothpaste used correctly.
The rice-grain/pea-sized rules exist specifically to prevent meaningful fluorosis risk. If you’re following those guidelines, you’re not causing harm.
That said, if your child is swallowing toothpaste regularly, using adult toothpaste (much higher fluoride concentration), and drinking heavily fluoridated water, the cumulative intake could become a concern worth discussing with your dentist.
It’s a real thing to be aware of. It’s not a reason to eliminate fluoride.
Common Mistakes Parents Make (I Made Some of These)

Using too much toothpaste. I’ve seen parents load up a toddler’s brush like they’re prepping an adult for a full brush session. A rice-grain smear for under 3, a pea for 3 to 6. That’s it.
Skipping fluoride toothpaste to “play it safe.” This is counterproductive. Fluoride-free toddler toothpaste does essentially nothing to prevent cavities. The safety concern people have is about overconsumption not about fluoride itself being harmful at appropriate doses.
Not brushing before bed. Night time is when fluoride matters most. Saliva production drops during sleep, which means the mouth’s natural defense against acid drops too. Brushing with fluoride toothpaste before bed and not eating or drinking anything afterward (except water) gives fluoride its best working window.
Not flossing at all. Fluoride in toothpaste doesn’t reach between teeth. If your child has teeth that touch each other, you need to be flossing regularly. Interdental spaces are where cavities love to hide.
Assuming baby teeth don’t matter. Some parents figure cavities in baby teeth are no big deal since they’ll fall out anyway. But untreated decay in primary teeth can cause pain, affect chewing and speech development, and spread to adjacent teeth including the permanent ones underneath. Caring for baby teeth matters.
Questions to Ask Your Child’s Dentist
If you’re not sure where your child stands on fluoride, here are the exact questions worth raising at your next visit:
- Is my child at high, medium, or low risk for cavities? The answer changes what fluoride protocol makes sense.
- Do we need fluoride varnish every 3 months or every 6?
- What’s the fluoride level in our local water? Your dentist should know, or can look it up.
- Should my child use a fluoride rinse at home? Usually recommended for kids 6+ with cavity history.
- Is silver diamine fluoride appropriate for any existing decay we haven’t treated yet?
A good pediatric dentist will walk through all of this with you. If yours hasn’t, bring the questions they’ll appreciate the engagement.
A Note on Kids With Braces or Special Needs
If your child is in orthodontic treatment, fluoride becomes even more important. Brackets and wires create dozens of new spots where plaque accumulates and can’t be brushed away easily. White spot lesions early decalcification around bracket edges are one of the most common complications of orthodontic treatment, and they’re essentially preventable with consistent fluoride use.
Ask the orthodontist specifically about prescription-strength fluoride gel for home use. This is typically a 0.4% stannous fluoride gel used in a custom tray. Combined with regular brushing, it dramatically reduces white spot risk during treatment.
For children with special needs who may not tolerate brushing well or who have diets that are higher in processed foods, the risk-benefit calculation leans even more strongly toward professional fluoride treatments. Work with a pediatric dentist who has experience with special needs patients they’ll tailor the approach.
FAQs: Fluoride in Pediatric Dentistry
Q: Is fluoride safe for babies?
A: In the correct amounts, yes. A rice-grain smear of fluoride toothpaste starting at the first tooth is safe and recommended. The concern is overconsumption over time, not fluoride itself at appropriate doses.
Q: My toddler swallows toothpaste is that a problem?
A: Swallowing a rice-grain smear occasionally is not a safety concern. If they’re regularly swallowing larger amounts, scale back and work on teaching spitting. Watch your child during brushing until they reliably spit.
Q: Can I use fluoride-free toothpaste for my child?
A: The AAPD doesn’t recommend it for children at any meaningful cavity risk. Fluoride-free “training toothpastes” don’t offer real cavity protection. They’re fine for helping kids get used to brushing before teeth appear, but once teeth are present, switch to fluoride toothpaste in the correct amount.
Q: How often does my child need fluoride varnish at the dentist?
A: Typically every 6 months for low-risk kids, every 3 months for high-risk. Your dentist will assess based on your child’s cavity history, diet, home care routine, and water fluoride level.
Q: Does fluoride in water work as well as topical fluoride?
A: They work differently but complement each other. Fluoridated water provides systemic and topical exposure throughout the day. Toothpaste delivers a concentrated topical dose twice daily. Both together offer better protection than either alone.
Q: My child has white spots on their teeth is that fluorosis?
A: Maybe, but not necessarily. White spots can also result from trauma, illness during tooth development, or enamel hypoplasia. Have your dentist evaluate them they can usually tell the difference on examination. If it is mild fluorosis, it’s cosmetic only and doesn’t harm the tooth.
Final Thoughts
If I could go back to when my daughter was born and give myself one piece of dental advice, it would be this: start early, use the right amount, and actually show up to those six-month checkups.
Fluoride in pediatric dentistry isn’t complicated once you know the basics. Use a rice-grain smear from the first tooth, graduate to a pea-size at three, keep brushing at night, and let your dentist apply varnish regularly. That combination consistent, boring, unsexy is what actually prevents cavities.
The fear around fluoride is largely based on misunderstanding of dose. At the levels used in pediatric care, fluoride is safe, effective, and backed by decades of solid research. The CDC, the American Academy of Pediatrics, and the AAPD all agree on this.
Your child’s teeth even the baby ones are worth protecting. And fluoride, used correctly, is one of the most powerful tools you have to do it.
Related reading from Toothoria: