

Discovering a dark spot or blood blister vs melanoma in your mouth can trigger immediate anxiety. While a blister with blood in the mouth typically represents a harmless condition that heals within two weeks, oral melanoma is a serious cancer requiring urgent treatment. Understanding the critical differences between these two conditions can literally save your life.
Oral melanoma accounts for less than 2 percent of all melanomas but carries a poor prognosis when diagnosed late, with five-year survival rates ranging from 15 to 50 percent depending on stage. In contrast, a blood blister inside the mouth is benign, self-limiting, and poses no long-term health risks. The challenge lies in accurate differentiation, as both conditions can present as dark pigmented lesions.
This expert guide provides clear, evidence-based criteria to distinguish blood blisters from melanoma, helping you recognize when that concerning oral lesion requires immediate professional evaluation versus simple home management. Understanding these differences empowers you to respond appropriately and avoid potentially life-threatening diagnostic delays.
What Is Oral Melanoma? Understanding the Deadly Reality
Definition and Prevalence
Oral melanoma is a rare but aggressive malignancy arising from melanocytes (pigment-producing cells) in the oral mucosa. It represents:
Key statistics:
- Less than 2 percent of all melanoma cases
- Approximately 1.2 cases per 10 million people annually
- Most common in patients aged 40 to 70 years
- Slightly higher incidence in males
- Five-year survival rate of 15 to 50 percent
Common Locations for Oral Melanoma
Unlike blood blister in mouth that predominantly affects the soft palate and buccal mucosa, oral melanoma shows distinct location preferences:
Primary sites (in order of frequency):
- Hard palate and maxillary gingiva (40 percent)
- Buccal mucosa (15 percent)
- Mandibular gingiva (10 percent)
- Tongue (8 percent)
- Lips and floor of mouth (remaining cases)
This anatomical distribution differs significantly from blood mouth blisters, which favor the soft palate and areas subject to mechanical trauma.
Blood Blister vs Melanoma: Critical Diagnostic Differences
Comprehensive Comparison Table
| Characteristic | Blood Blister in Mouth | Oral Melanoma |
| Onset Speed | Sudden (1 to 4 hours) | Gradual (weeks to months) |
| Color Pattern | Uniform dark red, purple, or black | Irregular with multiple colors (brown, black, blue, red, white) |
| Border Definition | Smooth, well-circumscribed, regular | Irregular, asymmetric, poorly defined |
| Size at Discovery | Usually 5 to 20mm | Often exceeds 6mm and continues growing |
| Texture | Soft, fluid-filled, fluctuant | Firm, indurated, may be raised or flat |
| Pain Level | Mild to moderate, pressure-sensitive | Often painless in early stages |
| Bleeding | Only when ruptured | Spontaneous or with minimal trauma |
| Duration | Resolves in 7 to 14 days | Persists and progressively enlarges |
| Blanching | Does not blanch with pressure | Does not blanch |
| Ulceration | Only after rupture, heals quickly | May ulcerate, does not heal |
| Recurrence | May recur at different locations | Recurs at same location if incompletely removed |
| Associated Symptoms | Isolated lesion, no systemic signs | May have lymphadenopathy, weight loss, malaise |
The ABCDE Rule for Melanoma Detection
Apply this mnemonic when evaluating any pigmented oral lesion:
A for Asymmetry:
- Melanoma: One half does not match the other half
- Blood blister: Symmetrical, uniform dome shape
B for Border irregularity:
- Melanoma: Irregular, scalloped, or poorly defined edges
- Blood blister: Smooth, well-defined circular or oval border
C for Color variation:
- Melanoma: Multiple colors (tan, brown, black, red, white, blue)
- Blood blister: Uniform dark red to purple throughout
D for Diameter:
- Melanoma: Often larger than 6 mm and continues growing
- Blood blister: Variable size but remains stable after initial formation
E for Evolution:
- Melanoma: Changes in size, shape, color, elevation, or symptoms over weeks to months
- Blood blister: Rapidly reaches maximum size within 24 hours, then ruptures and heals
Understanding Blood Blister Inside Cheek: Benign Characteristics

Typical Presentation
A blood blister inside the cheek or other oral location exhibits predictable features:
Appearance characteristics:
- Sudden onset following minor trauma or without identifiable cause
- Tense, dome-shaped elevation
- Smooth, intact surface (unless ruptured)
- Uniform dark red, purple, or bluish-black color
- Size typically 3 to 30mm
- Single lesion (multiple simultaneous blisters are uncommon)
Natural History and Timeline
Inside the mouth, a blood blister follows a characteristic evolution:
Hours 0 to 4: Rapid formation and expansion to full size
Hours 24 to 48: Peak size maintained, may spontaneously rupture
Day 3 to 7: Gradual resorption if intact, or healing of erosion if ruptured
Day 7 to 14: Complete epithelial healing without scarring or pigmentation
This predictable timeline contrasts sharply with melanoma’s progressive growth pattern.
Oral Melanoma Warning Signs: When to Seek Immediate Care
Red Flags Requiring Urgent Evaluation
Absolute indications for professional examination:
- Persistence beyond 3 weeks (any pigmented oral lesion not healing)
- Progressive growth (lesion steadily increasing in size)
- Color changes (development of darker areas or multiple colors)
- Irregular borders (asymmetric shape with poorly defined margins)
- Spontaneous bleeding (bleeding without trauma)
- Ulceration without healing (non-healing ulcer in pigmented area)
- Firm texture (indurated or hard consistency)
- Lymph node enlargement (palpable, firm nodes in neck)
- Numbness or tingling (neurological symptoms)
- Recurrence at same site (pigmented lesion returning in identical location)
High-Risk Patient Populations
Certain individuals face elevated oral melanoma risk:
Risk factors include:
- Age over 50 years
- History of cutaneous melanoma
- Excessive sun exposure to lips
- Tobacco use (smoking or chewing)
- Heavy alcohol consumption
- Pre-existing oral pigmentation
- Immunosuppression
- Fair skin with tendency to burn
Diagnostic Approach: How Professionals Distinguish Blood Blister vs Melanoma
Clinical Examination Techniques
Dental and medical professionals use systematic approaches:
Visual inspection:
- Comprehensive oral examination under adequate lighting
- Assessment of lesion symmetry, borders, color, and diameter
- Evaluation of surrounding tissues for satellite lesions
- Documentation with clinical photography
Palpation assessment:
- Texture evaluation (soft and fluctuant versus firm and indurate)
- Mobility testing (mobile versus fixed to underlying structures)
- Regional lymph node examination
Diascopy testing:
- Application of clear glass slide with pressure
- Vascular lesions blanch; melanoma and blood blisters do not
- Helps differentiate from hemangiomas and vascular malformations
When Biopsy Becomes Necessary
Indications for tissue sampling:
Mandatory biopsy situations:
- Any pigmented lesion persisting beyond 14 to 21 days
- Lesions meeting two or more ABCDE criteria
- Progressive growth or color changes
- Firm, indurated texture
- Ulceration without apparent trauma
- Patient anxiety requiring definitive diagnosis
Biopsy techniques:
- Excisional biopsy for small lesions (less than 10mm) with 2 to 3 mm margins
- Incisional biopsy for larger lesions, sampling most suspicious area
- Histopathologic examination with immunohistochemistry
- Molecular testing if diagnosis uncertain
Management Differences: Blood Blister vs Melanoma Treatment
Blood Blister Treatment Approach
Conservative management for causes of oral blood blisters:
Home care strategies:
- Avoid intentional rupture or manipulation
- Saltwater rinses 4 to 6 times daily
- Soft diet avoiding trauma
- Topical anesthetics for comfort
- Cold compresses for pain and swelling
- Observation for expected resolution within 2 weeks
Professional intervention (rarely needed):
- Sterile drainage for large, functionally impairing lesions
- Investigation if recurrent (3 or more episodes in 6 months)
- Treatment of underlying causes (nutritional deficiencies, medication adjustment)
Melanoma Treatment Requirements
Aggressive multidisciplinary approach:
Surgical management:
- Wide local excision with 1 to 2 cm margins
- Sentinel lymph node biopsy to assess spread
- Neck dissection if lymph node involvement confirmed
- Possible maxillectomy or mandibulectomy for bone invasion
Adjuvant therapies:
- Immunotherapy (pembrolizumab, nivolumab)
- Targeted therapy for specific mutations (BRAF, MEK inhibitors)
- Radiation therapy for high-risk or unresectable cases
- Chemotherapy in advanced stages
Prognosis factors:
- Tumor thickness (Breslow depth)
- Presence of ulceration
- Mitotic rate
- Lymph node involvement
- Distant metastases
Black Blister on Lip: Special Considerations

External Oral Lesions
A black blister on the lip requires particular attention due to high sun exposure and visibility:
Benign causes:
- Traumatic blood blister from lip biting
- Angiokeratoma (vascular lesion)
- Venous lake (blanches with pressure)
- Melanotic macule (flat, stable pigmentation)
Concerning features suggesting melanoma:
- Asymmetric growth pattern
- Border irregularity
- Color variegation
- Diameter exceeding 6 mm
- Evolution over time
- Located on sun-exposed lower lip (highest risk site)
Critical point: Lip melanoma carries a particularly poor prognosis due to rich lymphatic drainage and a tendency for early metastasis. Any suspicious pigmented lip lesion warrants immediate dermatologic or oral surgical evaluation.
Prevention and Early Detection Strategies
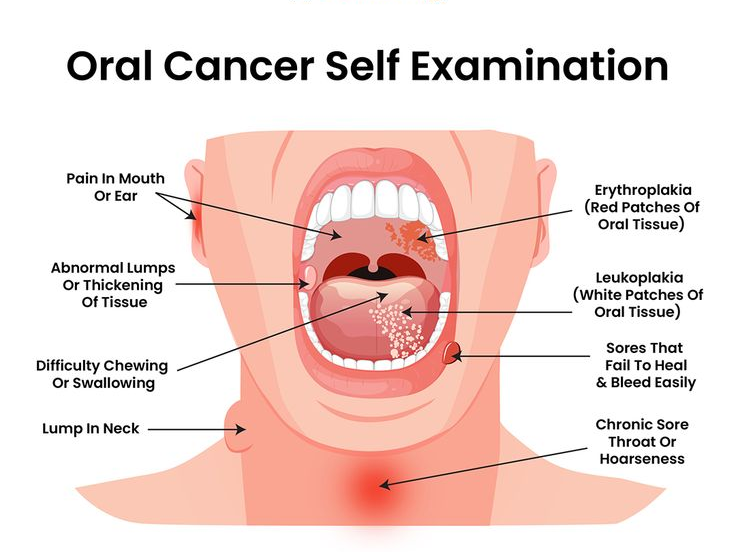
Monthly Self-Examination Protocol
Systematic oral self-screening:
- Use good lighting and a mirror.
- Examine lips (outer and inner surfaces)
- Inspect cheeks, gums, and palate
- Check tongue (top, bottom, sides)
- Evaluate floor of mouth and throat
- Note any new or changing pigmented areas
- Document with smartphone photos for comparison
Professional Screening Recommendations
Routine dental examinations:
- Annual comprehensive oral cancer screening
- High-risk patients: every 6 months
- Dentist evaluation of any suspicious lesions
- Referral to oral surgeon or dermatologist when indicated
Frequently Asked Questions
How can I tell the difference between a blood blister vs melanoma?
Blood blisters appear suddenly within hours, have a uniform dark red or purple color, have smooth borders, and heal within 7 to 14 days. Melanoma develops gradually over weeks to months, shows irregular borders with multiple colors, feels firm, and continues growing without healing.
What does oral melanoma look like in early stages?
Early oral melanoma appears as a flat or slightly raised brown or black spot with irregular borders, asymmetric shape, and variable coloring. It may be painless initially and located most commonly on the hard palate or upper gums.
When should I see a doctor for a dark spot in my mouth?
See a doctor immediately if any pigmented oral lesion persists beyond 3 weeks, grows larger, changes color, has irregular borders, bleeds spontaneously, or feels firm and fixed to underlying tissue.
Can a blood blister in the mouth turn into melanoma?
No, a blood blister inside the mouth cannot transform into melanoma. They are completely different conditions with different cellular origins. Blood blisters are benign trauma-related lesions, while melanoma is a malignant tumor of melanocytes.
How common is oral melanoma?
Oral melanoma is rare, representing less than 2 percent of all melanomas, with approximately 1.2 cases per 10 million people annually. It occurs most commonly in patients aged 40 to 70 years.
What is the survival rate for oral melanoma?
Five-year survival rates for oral melanoma range from 15 to 50 percent depending on the stage at diagnosis. Early detection and treatment significantly improve outcomes, making prompt evaluation of suspicious lesions critical.
Does a black blister on the lip mean cancer?
Not necessarily. Most black blisters on lips are traumatic blood blisters that heal within two weeks. However, any pigmented lip lesion persisting beyond 3 weeks, especially with irregular features, requires professional evaluation to rule out melanoma.
How fast does oral melanoma grow?
Oral melanoma typically grows slowly over weeks to months, though growth rates vary. Unlike blood blisters that reach maximum size within 24 hours, melanoma shows progressive enlargement without spontaneous resolution.
Conclusion:
Understanding blood blister vs melanoma differences empowers you to make informed decisions about oral lesions. While most dark spots in the mouth represent harmless blood blister in mouth formations that resolve spontaneously, the potentially deadly nature of oral melanoma demands vigilance and appropriate professional evaluation when warning signs appear.
The key takeaway: any pigmented oral lesion persisting beyond 3 weeks, exhibiting irregular features, or causing concern warrants immediate professional examination. Early detection of melanoma dramatically improves survival rates, making timely evaluation crucial. Conversely, recognizing typical blood blister inside cheek characteristics allows confident home management without unnecessary anxiety or medical expenses. When in doubt, always err on the side of professional assessment because distinguishing a blood blister vs melanoma can literally be a matter of life and death.
e